Acid reflux, that irritating backflow of stomach acid up into your esophagus, is often triggered by what you eat and drink. Eat the wrong food, and you’re sure to feel the burn. Some foods are known to cause reflux more than others.
Eating the right foods will help lessen symptoms and the need for medications.
Symptoms of GERD
• Burning sensation in the chest and upper abdomen
• Bitter taste in the mouth
• Trouble swallowing
• Chronic coughing
• Hoarseness
• A feeling that something is stuck in the throat.
One of the underlying reasons for GERD is a weakened lower esophageal sphincter (LES) present between the stomach and esophagus. This sphincter normally prevents acid from coming back into the esophagus2.
What foods should be eaten?
Some foods can even help to reduce GERD symptoms.
Studies shows that Mediterranean diets, which are rich in fruits, vegetables, fiber, whole grains, and unsaturated fats, play an excellent role in lessening GERD severity.
- The lower esophageal muscle can be weakened by factors other than food. The following recommendations may help reduce symptoms:
1. Stop using tobacco in all forms. Nicotine weakens the lower esophageal muscle.
2. Avoid chewing gum and hard candy. They increase the amount of swallowed air which, in turn, leads to belching and reflux.
3. Do not lie down immediately after eating. Avoid late evening snacks.
4. Avoid tight clothing and bending over after eating.
5. Eat small, frequent portions of food and snack if needed.
6. Lose weight if overweight. Obesity leads to increased reflux.
7. Elevate the head of the bed six to eight inches to prevent reflux when sleeping. Extra pillows, by themselves, are not very helpful.
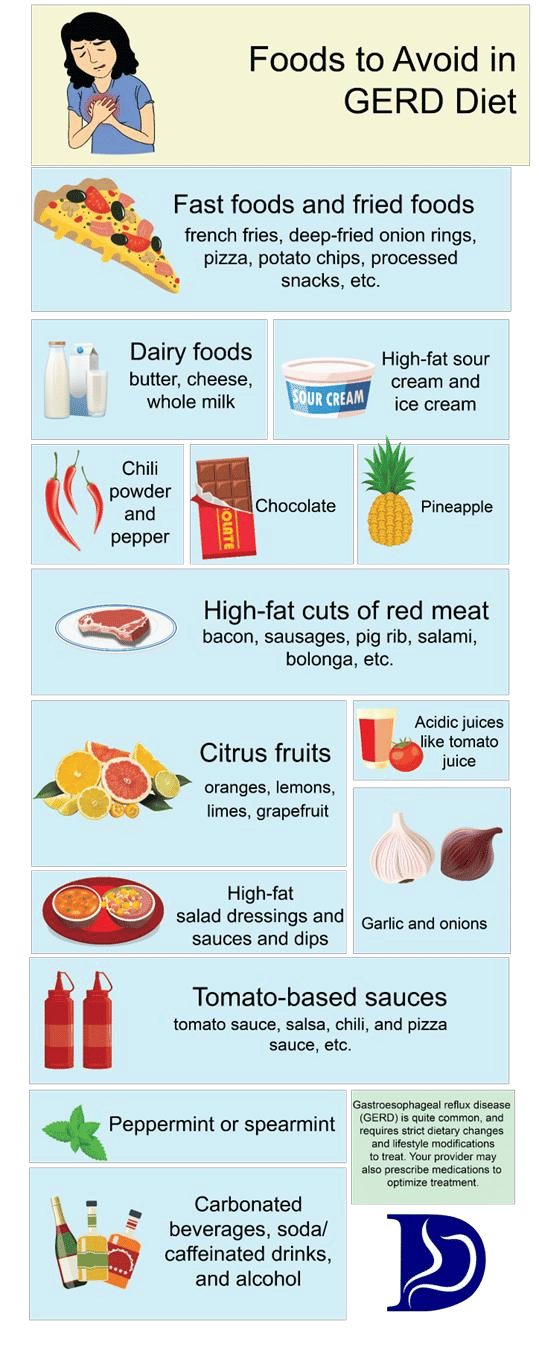
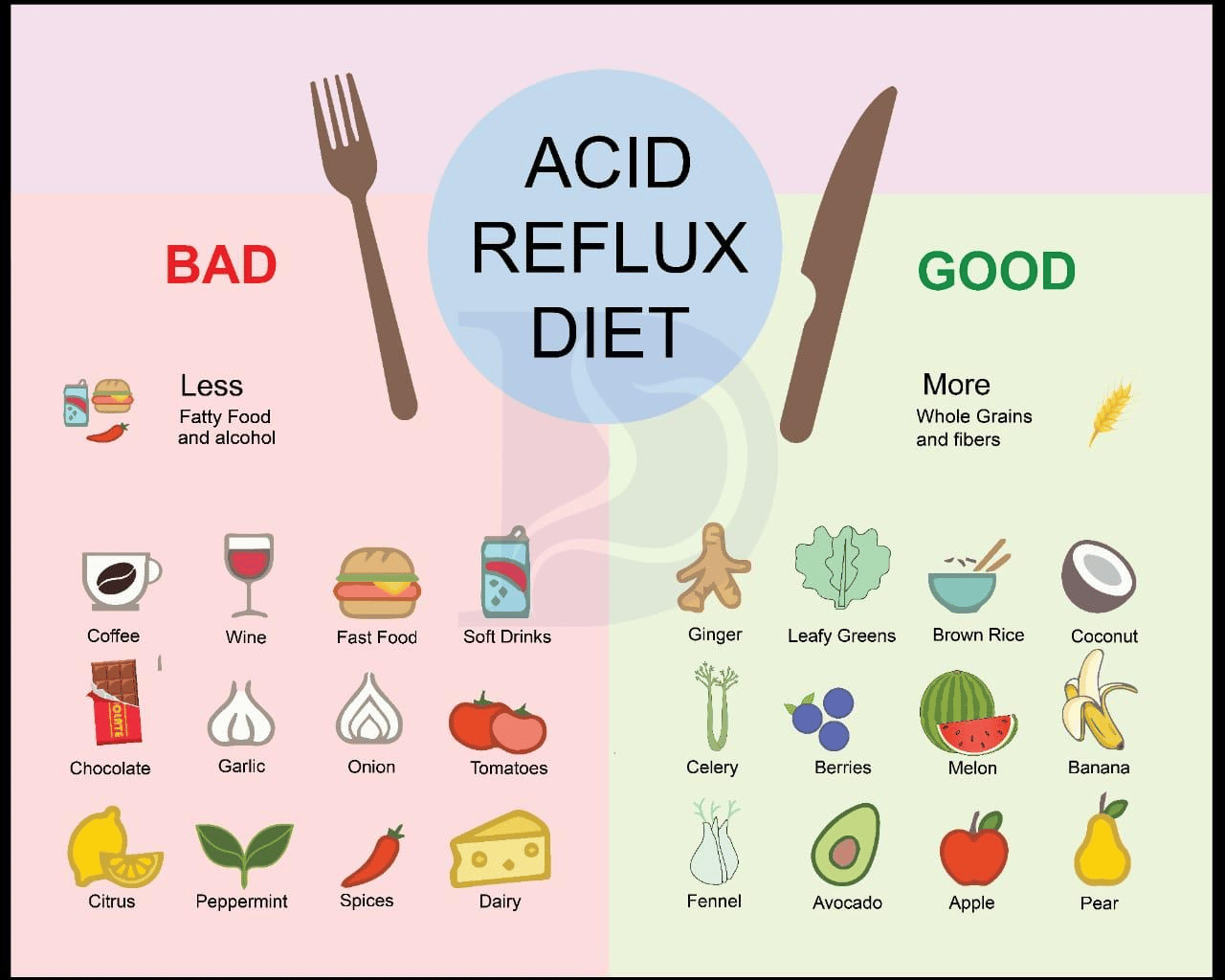
- The following foods aggravate acid reflux and should be avoided: ▪ fatty or fried foods ▪ peppermint and spearmint ▪ whole milk ▪ oils ▪ chocolate ▪ creamed foods or soups ▪ most fast foods The following foods irritate an inflamed lower esophagus and may need to be limited or avoided: ▪ citrus fruits and juices (grapefruit, orange, pineapple, tomato) ▪ coffee (regular and decaffeinated) ▪ caffeinated soft drinks ▪ tea ▪ other caffeinated beverages Some individuals may not tolerate spicy or acidic foods
| Food Groups | ||
|---|---|---|
| Group | Recommend | Avoid |
| Milk or milk products | skim, 1% or 2% low-fat milk; lowfat or fat-free yogurt | whole milk (4%), chocolate milk |
| Vegetables | all other vegetables | fried or creamy style vegetables*, tomatoes |
| Fruits | apples, berries, melons, bananas, peaches, pears | citrus*: such as oranges, grapefruit, pineapple |
| Bread & grains | all those made with low-fat content | any prepared with whole milk or high fat content |
| Meat, meat substitutes | low-fat meat, chicken, fish, turkey | cold cuts, sausage, bacon, fatty meat, chicken fat/skin |
| Fat, oils | none or small amounts | all animal or vegetable oils |
| Sweets & desserts | all items made with no or low fat (less than or equal to 3 g fat/serving) | chocolate, desserts made with oils and fats |
| Beverages | decaffeinated, non-mint herbal tea; juices (except citrus); water | alcohol, coffee (regular or decaffeinated), carbonated beverages, tea, mint tea |
| Soups | fat-free or low-fat based | chicken, beef, milk, or cream-based soups |
| *Individually determined | ||
Summary
Chronic gastroesophageal reflux may cause complications like esophagitis, laryngitis, tooth enamel erosions, and heartburn. Apart from medication, the most effective way to manage GERD is with dietary modification.
References
1. Kellerman R, Kintanar T. Gastroesophageal Reflux Disease. Prim Care. 2017;44(4):561- 573. doi:10.1016/J.POP.2017.07.001
2. Grossi L, Ciccaglione AF, Travaglini N, Marzio L. Transient lower esophageal sphincter relaxations and gastroesophageal reflux episodes in healthy subjects and GERD patients during 24 hours. Dig Dis Sci. 2001;46(4):815-821. doi:10.1023/A:1010708602777
3. Wu P, Zhao XH, Ai ZS, et al. Dietary intake and risk for reflux esophagitis: A casecontrol study. Gastroenterol Res Pract. 2013;2013. doi:10.1155/2013/691026